The private-sector paradox
South Africa’s private healthcare sector possesses all the necessary ingredients for world-class disease management. Yet, a profound paradox remains: funding care is fundamentally different from controlling disease. Because these independent elements have not been integrated into a cohesive, population-level control system, the actual tracking of blood pressure control falls into a major visibility gap, leaving patients exposed to preventable long-term harm.
14 July 2026
9.7 min read
In theory, hypertension should be easier to control in the insured population than in the country as a whole. Here are three reasons:
- Hypertension is a Prescribed Minimum Benefit (PMB). For medical scheme members, this means access to doctors, pharmacies, pathology services, antihypertensive medicines and related chronic disease benefits.
- The condition is common, measurable and, for most patients, treatable with well-established lifestyle and pharmacological interventions.
- If not well controlled, it is closely linked to costly downstream events, including stroke, heart failure and kidney disease.[1,6]
The private sector should therefore have both the means and the motivation to organise reliable long-term control of hypertension.
The evidence suggests a more complicated picture.
Limited public data, mixed signals
An analysis of the first South African Demographic and Health Survey, published in 2008, found that people with medical aid were significantly more likely to be on treatment and to have controlled blood pressure than those without it. People without medical aid had about 40% lower odds1 of having controlled blood pressure. This is useful as a historical signal, but it used 1998 data, relied on medical aid membership as a proxy for private-sector care, and applied an older control threshold. It should therefore not be treated as a current private-sector benchmark. [2]
More recent data from Discovery Health point to a persistent problem. Discovery reported hypertension prevalence of 18.4%, awareness of 68.7%, and control of only 26.1%. In the same context, hypertension prevalence rose 22% over five years, and new diagnoses among members aged 25–39 increased by about 5% per year. [3,7]
Some schemes have programme elements related to cardiovascular risk and chronic disease management. Discovery’s Cardio Care is an example. Many other schemes run chronic disease-management or integrated-care programmes. These are important, but they do not amount to a visible population-level hypertension control system.
Funding care is not the same as controlling disease.
Schemes and administrators can usually see claims, consultations, medicine dispensing, pathology use, chronic registrations and other administrative signals. These data are useful, but they do not necessarily show whether a member’s blood pressure is controlled, uncontrolled, unknown, or worsening over time.
Hypertension is a longitudinal follow-through challenge, not simply an authorisation problem.
This is where the hypertension care cascade (Figure 1) is useful. It tracks the proportion of people with hypertension who are diagnosed, treated and controlled. Expanded versions also include screening, linkage to quality care, persistence and monitoring. The cascade is useful because it shows both success and failure: identifying the numbers who reach control, whose control status is unknown, and where people disappear from the pathway. [8]
For an insured population, the cascade raises several practical questions:
- How many members likely have hypertension?
- How many have been diagnosed?
- How many are registered for chronic benefits or disease management programmes?
- How many are actively treated?
- How many have stayed on treatment a year later?
- How many have enough blood pressure data to classify control?
- How many are controlled, uncontrolled or of unknown control status?
A mature chronic care system should be able to answer these questions. If it cannot, that in itself is an important finding.
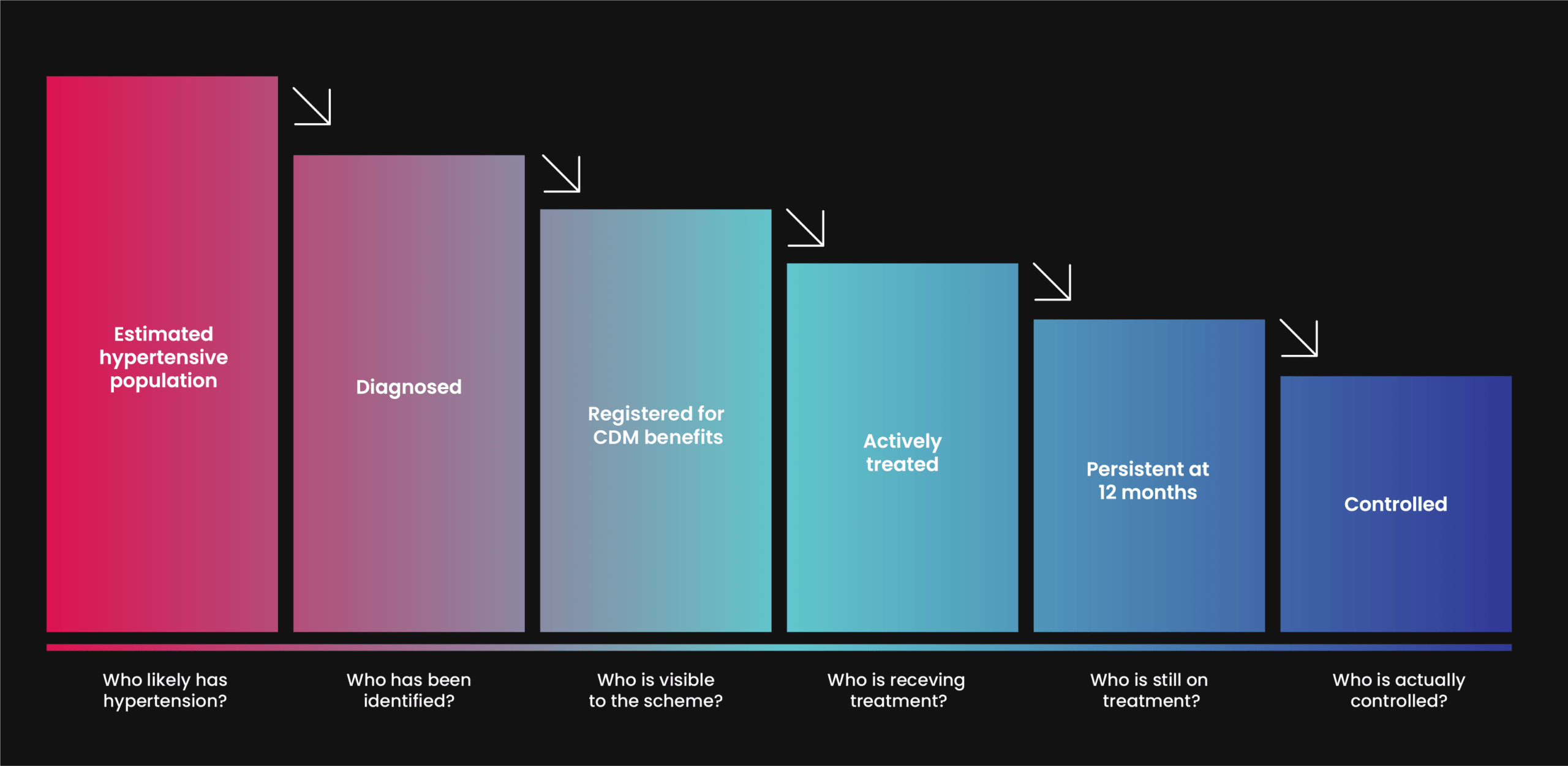
Figure 1. The hypertension care cascade in an insured population. A framework for identifying patients lost to care, from the initial stages of likely hypertension through to diagnosis, treatment, follow-up and control.
The 2019 Health Market Inquiry made the point that outcomes are what ultimately matter to patients and, when combined with cost data, are essential for measuring value. The inquiry also highlighted the importance of access and found that reliable, comparable and meaningful outcomes information was lacking in the private healthcare market. [4]
Hypertension is a good example of why this matters.
The denominator
The challenge starts with the denominator: identifying how many members actually have hypertension.
In medical scheme populations, hypertension prevalence is not as simple as it first appears. The number of people formally registered for chronic benefits may be lower than the number whose claims records suggest hypertension.
A useful distinction therefore is between registered prevalence and apparent prevalence. Registered prevalence captures people formally enrolled in chronic medicine or disease-management structures. Apparent prevalence is broader and can be inferred from claims patterns, ICD-10 coding, medicine use and other data signals. [5]
In a 2022 analysis of South African medical scheme data, hypertension had a registered prevalence of 16.6%. When stricter entry and verification criteria were applied, the estimate fell to 9.1%. The important point is not which number is “correct”; it is that different definitions produce very different pictures of the hypertensive population. [5]
This is more than a technical point. Disease prevalence is the foundation for population management, risk adjustment, forecasting and quality measurement. If the denominator is wrong, almost every downstream performance signal is affected: control rates, medication refill gaps, complication rates and programme reach. [5]
The role of GPs
General practitioners and family physicians are central to any realistic hypertension strategy. They diagnose the condition, assess cardiovascular risk, decide when lifestyle measures are insufficient, start treatment, intensify treatment and refer patients whose hypertension is resistant, suspicious for a secondary cause, or otherwise more complex. Any model that sidelines general practice would be poorly designed. [1,6]
But the centrality of GPs does not mean that practices can carry the entire burden alone. Population-level hypertension control requires capabilities that many practices struggle to sustain by themselves: defining the hypertensive population, identifying uncontrolled patients, tracking medicine refill gaps, arranging follow-up, incorporating home blood pressure readings and escalating care when control is not achieved. This is where scheme, administrator and managed-care infrastructure should help.

The private-sector problem is weak system integration
The system contains many capable actors, but it does not automatically behave like a coherent hypertension control system.
The actors with the largest long-term financial stake in preventing stroke, heart failure and dialysis are not usually the ones making day-to-day clinical decisions. Clinicians doing the day-to-day work are not always supported with registries, dashboards, recall tools or control-status reporting.
Pharmacies and retail clinics may improve convenient access to blood pressure measurement, but convenience alone does not produce control unless elevated readings reliably trigger confirmation, treatment adjustment, follow-up or referral.
This matters even more because hypertension is closely linked to obesity, dyslipidaemia, diabetes, chronic kidney disease and cardiovascular disease.
The private sector needs more than a better hypertension programme, it needs a better chronic care model.
A narrow vertical solution devoted only to hypertension may improve a few metrics, but it risks adding one more pathway to an already fragmented patient journey.
Measurement as a starting point
A better starting point would be to make hypertension more measurable: generating clearer denominators, more complete blood pressure data, reporting of control status, and tracking of medication refill gaps.
In well-organised systems, hypertension control is a formal quality measure.
In the United States, for example, the “Controlling High Blood Pressure” measure assesses the percentage of hypertensive patients aged 18–85 whose most recent blood pressure is below 140/90 mmHg. [9]
South Africa’s private sector does not make an equivalent measure routinely visible. The absence of such a routinely visible measure is part of the problem.
Summary
The private sector has many of the ingredients required for better control: funding mechanisms, clinical capacity, chronic medicine benefits, pharmacies, data systems, managed-care infrastructure and member-facing communication channels. The paradox is that these ingredients have not necessarily been assembled into a functioning hypertension control system. As a result, the care pathway breaks down in several places.
Where this happens and how it could be reinforced is the subject of the next article.
References
[1] Council for Medical Schemes. PMB / CDL resources for hypertension coverage. https://www.medicalschemes.co.za/resources/pmb
[2] Steyn K, Bradshaw D, Norman R, Laubscher R. Determinants and treatment of hypertension in South Africans: the first Demographic and Health Survey. S Afr Med J. 2008;98(5):376–380. Available from: https://pubmed.ncbi.nlm.nih.gov/18637309/
[3] Discovery scheme update on prevalence growth and rise in diagnoses https://www.mynewsdesk.com/za/discovery-holdings-ltd/pressreleases/discovery-health-medical-scheme-notes-an-increase-in-young-people-diagnosed-with-chronic-high-blood-pressure-hypertension-3322821
[4] Competition Commission Health Market Inquiry final report. https://www.compcom.co.za/wp-content/uploads/2020/01/Final-Findings-and-recommendations-report-Health-Market-Inquiry.pdf
[5] Bennett. “Who’s got what? A closer look at disease prevalence”. Registered vs apparent prevalence and why denominators matter. https://www.actuarialsociety.org.za/convention/wp-content/uploads/2024/11/2024-ASSA-Bennett-FIN.pdf
[6] WHO hypertension fact sheet for broader global framing and measurable control logic. https://www.who.int/news-room/fact-sheets/detail/hypertension
[7] Discovery Health Insights – Discovery, accessed April 18, 2026, https://www.discovery.co.za/portal/corporate/health-insights-how-healthy-is-our-nation
[8] Benade M, et al. Health systems performance for hypertension control using a care cascade approach in South Africa, 2008–2017. PLOS September 7, 2023
[9] Centers for Medicare & Medicaid Services. Quality ID #236: Controlling High Blood Pressure. 2025. Available from: https://qpp.cms.gov/docs/QPP_quality_measure_specifications/CQM-Measures/2025_Measure_236_MIPSCQM.pdf
Get an email whenever we publish a new thought piece
Hypertension care is often a series of disconnected events. Blood pressure is measured, advice is given, a prescription is written, and follow-up is advised. The patient disappears back into everyday
8.2 min read

If hypertension is common, measurable and treatable, why do so many patients still have uncontrolled blood pressure? Drug shortages, diagnostic challenges or a lack of treatment guidelines are not the
10.6 min read
Meet our experts
Author

More Insights
Focused Thought Pieces