Hypertension is a test of whether healthcare is measuring what matters
Hypertension Awareness Month offers an important reminder that high blood pressure is one of the most common, measurable and consequential health risks facing our country and our healthcare system.
28 May 2026
10.5 min read
World Hypertension Day, observed annually on 17 May, focuses public attention on prevention, detection and control. But for healthcare funders, administrators, clinicians and policymakers, hypertension also raises a deeper question: are we measuring the activity of healthcare, or the outcomes that matter?
High blood pressure is closely linked to stroke, heart failure, kidney disease and premature death, yet it is often silent in its early stages. This makes awareness important. It also makes system performance critical. World Hypertension Day is part of Hypertension Awareness Month which is focused on prevention, detection and control at individual, community and health-system levels.
Hypertension can also be read as a test of healthcare system performance.
The reason is this: unlike many other health challenges, hypertension is easy to measure, well understood and usually treatable. Blood pressure can, at minimal cost, be checked, effective medicines have been available for decades and clinical targets are well defined. In theory, this makes hypertension a condition well suited to organised, long-term management.
The burden of uncontrolled hypertension
The World Health Organisation estimates that hypertension affects about 1.4 billion adults aged 30 to 79, with a significant proportion unaware that they have a condition that causes over 10 million deaths each year. And, globally, even when diagnosed, blood pressure control is often poor. South Africa carries a major burden too, with raised blood pressure contributing to 12.5% of deaths annually via stroke, cardiovascular and renal disease. This is a major clinical concern but also an issue of quality, cost and health system design.

The gap between access and control
In the insured healthcare environment, medical scheme members generally have access to doctors, medicines, pathology services, pharmacies and chronic disease benefits. Hypertension is included on the Chronic Disease List (CDL) within Prescribed Minimum Benefits (PMB). This means that the ingredients for better control are present, at least on paper.
The question is whether the available ingredients add up to a functioning hypertension control system.
Healthcare systems can usually measure activity. In other words, they can count consultations, prescriptions, chronic medicine registrations and pharmacy transactions. These utilisation signals are important, but they do not show whether blood pressure is controlled, whether patients have fallen off the treatment pathway, or whether treatment needs to be intensified.
Funding care is not the same as controlling disease. This distinction
applies to the overall care of patients with chronic disease.
Why healthcare systems struggle to function as integrated systems
The healthcare system has many capable actors, and this is not a judgment against any one of them. GPs diagnose, prescribe, adjust treatment and, where necessary, refer. Schemes, administrators and managed care organisations fund care, design benefits, and provide data infrastructure. Pharmacies and retail clinics expand access. Specialists manage resistant or complex hypertension.
The challenge is that these capable actors do not necessarily operate as a coherent system. The parties carrying much of the downstream financial risk are not closest to day-to-day clinical decisions. Clinicians doing the practical work of care are not always supported with registries, patient recall systems, medication refill-gap alerts or disease control-status reporting that they would need to manage hypertension reliably and at scale.
The result is that a patient may be diagnosed, receive a prescription, generate claims for payment and still not achieve sustained control of their blood pressure. From the outside, the system appears to be working. Gaps are only visible years later when uncontrolled blood pressure contributes to stroke or heart failure, kidney disease, disability and avoidable hospitalisation.
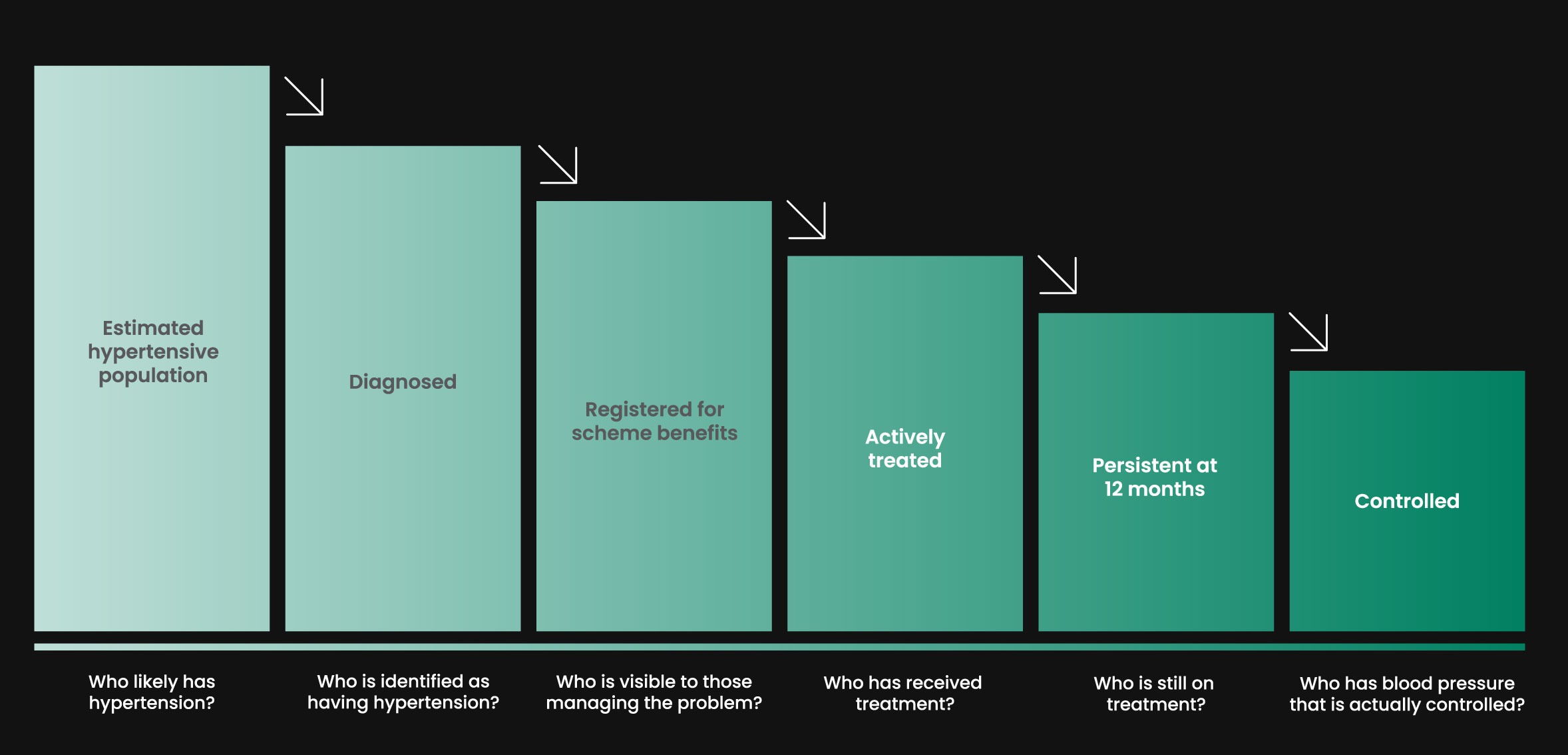
The Hypertension Care Cascade
The hypertension care cascade depicted below asks a number of practical questions. How many people in the population are likely to have hypertension? How many have been diagnosed? How many are being treated? How many are still on treatment a year later? How many have enough blood pressure data to classify their degree of control? And, finally, how many have blood pressure that is actually controlled?
A mature chronic care system should be able to answer these questions. If it cannot, this is a signal that clinicians and managers do not have the visibility needed to properly manage a common and consequential condition.
Outcomes, value and accountability in healthcare
Outcomes are what matter most, and when linked to cost, they are central to understanding value in healthcare. The Health Market Inquiry made this point in relation to South Africa’s private healthcare sector, noting the importance of reliable, comparable and meaningful outcomes information. For hypertension, this means looking beyond whether care was authorised or paid for to ask whether the condition was controlled over time.
The question is not only whether care was authorised or paid for. It is whether the condition was controlled over the long term.
The importance of integrated chronic care
Often, hypertension is not the patient’s only health condition. Multimorbidity is common, particularly later in life. Hypertension is linked to diabetes, abnormal lipids, obesity-related disease, chronic kidney and vascular disease.
A stand-alone hypertension programme might improve selected metrics but could further complicate and fragment the care system. The bigger opportunity is to develop a chronic care model that can manage overlapping and cuncurrent conditions and risk.
This is critical for patients because better follow-through means less of the preventable complications of hypertension that devastate lives. It matters for clinicians, because good care is easier to deliver with tools that support continuity. It is important for funders and administrators, because avoidable downstream events are costly. And it is critical for the health system as a whole because chronic disease drives much of the long-term burden of illness, disability and cost.
What better hypertension care requires
Better hypertension care does not require drastic reinvention of care, rather it requires common and basic things to be done consistently well.
- Elevated blood pressure readings need to be confirmed
- Treatment should start when it is indicated
- Lifestyle and cardiometabolic risk support should be integrated into care
without delaying medication when medication is needed - Treatment should be simplified wherever possible and intensified when
control is not achieved - Follow-up should be planned, not left to chance
- Blood pressure monitoring, including measurement at home, should feed into
action, not simply produce numbers - Patients whose hypertension is resistant, complex or linked to other risks need
well defined referral pathways
Much of this depends on information infrastructure including well defined population denominators, more complete blood pressure data, patient registries, patient recall systems, and reporting on medication refill-gaps and hypertension control-status. These elements need to be in feedback loops that show clinicians and funders where the pathway is working – and where patients are being lost to follow-up care.

Building a coordinated system around outcomes
Improving hypertension management requires better coordination between schemes, administrators, providers, pharmacies and clinicians. It requires the ability to identify the population at risk, classify control, support follow-up, recognise more complex conditions required specialist care and, fundamentally, to intervene before expensive and irreversible harm occurs.
To improve overall healthcare system design and delivery, hypertension is a good place to start because it is so common, measurable and consequential and because the private healthcare sector already has many of the ingredients needed for better control. These assets now need to be better connected around a shared outcome.be better connected around a shared outcome.
What better hypertension control will take
This can happen if medical schemes, administrators, clinicians, pharmacies and managed care organisations treat hypertension control as a system-level priority.
This means agreeing on the measures that matter, and building registries and feedback loops that make blood pressure control visible as an outcome over the long term. If we can do this for hypertension, we will have evidence that South African private healthcare is not only paying for activity but organising itself for better health.
Sources:
- World Health Organization. Hypertension fact sheet.
https://www.who.int/news-room/fact-sheets/detail/hypertension - Peer N, et al. National analyses of hypertension prevalence in South Africa.
https://www.sciencedirect.com/science/article/pii/S2590113321000171 - Nojilana B, Bradshaw D, Pillay-van Wyk V, et al. Estimating the changing burden of disease attributable to high systolic blood pressure in South Africa for 2000, 2006 and 2012. S Afr Med J. 2022.
https://samajournals.co.za/index.php/samj/article/view/219
https://www.ajol.info/index.php/samj/article/view/233870/220883 - National Department of Health, Statistics South Africa, SAMRC, ICF. South Africa Demographic and Health Survey 2016.
https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf - Bradshaw D, et al. Second Comparative Risk Assessment for South Africa. S Afr Med J 2022;112(8b):556-570.
https://doi.org/10.7196/SAMJ.2022.v112i8b.16648 - National Department of Health. National User Guide on the Prevention and Treatment of Hypertension.
https://knowledgehub.health.gov.za/system/files/elibdownloads/2023-04/HYPERTENSION%2520USER%2520GUIDE%2520FINAL%2520COPY.pdf
- Council for Medical Schemes. Prescribed Minimum Benefits and Chronic Disease List resources.
https://www.medicalschemes.co.za/resources/pmb/ - Competition Commission South Africa. Health Market Inquiry Final Findings and Recommendations Report.
https://www.compcom.co.za/wp-content/uploads/2020/01/Final-Findings-and-recommendations-report-Health-Market-Inquiry.pdf - Benade M, et al. Health systems performance for hypertension control using a care cascade approach in South Africa, 2008–2017. PLOS Global Public Health. 2023.
https://doi.org/10.1371/journal.pgph.0002055 - World Health Organization. HEARTS technical package for cardiovascular disease management in primary health care.
https://www.who.int/publications/i/item/WHO-NMH-NVI-18-14 - World Health Organization. Guideline for the pharmacological treatment of hypertension in adults.
https://www.who.int/publications/i/item/9789240033986
Get an email whenever we publish a new thought piece
If hypertension is common, measurable and treatable, why do so many patients still have uncontrolled blood pressure? Drug shortages, diagnostic challenges or a lack of treatment guidelines are not the
10.6 min read

In theory, hypertension should be easier to control in the insured population than in the country as a whole. Here are three reasons: Hypertension is a Prescribed Minimum Benefit (PMB).
7.3 min read
Meet our experts
Author

More Insights
Focused Thought Pieces