Closer to Home: The Affordable Care Act and NHI
29 August 2017
7.3 min read
By Gary Kantor
The battle between Democrats and Republicans over the Affordable Care Act (ACA) – Obamacare – is of interest to observers worldwide. Despite obvious differences between South African and US health care systems, the unfolding drama there may be relevant to health care policy makers locally as we consider our own high stakes health reform initiative, NHI – National Health Insurance.
The failure to achieve universal health coverage in the United States despite the country’s wealth and its enormous total national spend on health care, (around 18% of GDP – over $3 trillion) marks it out as different from other developed nations. Americans still struggle over the principle of equity, arguing whether health care is a universal entitlement or can be treated as a set of market-driven services. By contrast, the public discourse in SA is much more aligned with the rest of the world which tends to regard the provision of universal, equitable access to decent health care as a societal responsibility.
Public debate in the US, like our own, has focused mainly on access (cover), finance and cost. Obamacare, a legislative package that was passed in 2010, significantly reformed health insurance, driven by the administration’s intention of making sure all citizens would be covered. Despite Republican protestations, and multiple attempts to derail it legislatively during Obama’s tenure, and now Trump’s, Obamacare has been successful in that many more Americans – around 22 million more – are now guaranteed access to insurance despite pre-existing health conditions and/or low income. The ACA also introduced community rating (a long-standing principle in South Africa which inhibits pricing based on individual health status), subsidised expansion of the publicly funded Medicaid program, which supports low-income individuals and families, and created insurance exchanges (markets) in which private insurance could be purchased by individuals and small groups lacking access to employer-sponsored insurance. Obamacare also gave people better cover, for example first-dollar reimbursement for preventive care, and new prescription-drug benefits. Finally, the ACA imposed requirements on insurance companies for transparency about premium increases, and capped overhead (non-healthcare) expenses to about 15% of the total.
Most important, but often lost in the current debate both here and in the US, is that health policy, hence health system reform, should consider not only access, finance and cost but how well care is actually delivered. In fact, Obamacare did put in place a number of important programs and initiatives to redesign health care delivery that we in South African would do well to study. Don Berwick, one of the main architects and implementers of Obamacare during his time as the head of the publicly funded Medicare and Medicaid programs (CMS) (2016 budget – $957 billion) refers to these aspects of ACA as the “better care” law (Figure 1). It has three focus areas.
First, ACA introduced initiatives to integrate care – to support better teamwork across inpatient and outpatient settings, and diminish the known negative effects, on cost and quality, of traditional silos of care. For example, the legislation paved the way for so-called Accountable Care Organisations (ACOs) in which hospitals and physician groups can work together in an integrated manner. Bundled payments were introduced, for example a single payment to hospitals and doctors for total joint replacements, again with the hope of better planned, more coordinated care, and improved outcomes at lower cost because of the incentive to avoid costly complications. Special programs were introduced for some of the most vulnerable publicly-insured patients and to support transitions of care e.g. from hospital back into the community. Such transitions are known to be weak points in health care systems, resulting, when poorly managed, in unnecessary, recurrent hospitalisations and undesired, expensive days away from home and family. It is noteworthy that Accountable Care Organisations could not exist in SA as they would fall foul of regulations governing the health professions.
Second, Obamacare has driven a greater emphasis on quality. For example the ACA introduced new quality metrics, and greater transparency around outcomes. These measurements facilitate reimbursement innovations such as paying more for better outcomes of care, and for reduced complications – so-called value-based payment. Obamacare has also driven a lot of work to detect and prevent fraud and abuse. In South Africa there have been several calls from around the industry, including from the Health Market Enquiry, for greater transparency and reporting of quality measures and outcomes. National Core Standards cover certain aspects of quality but do not directly address the options for measuring and reporting health outcomes.
Third, the ACA lead to significant investment in innovation. The Center for Medicare and Medicaid Innovation (CMMI) was given $10Bn over a 10-year period for example to focus on teamwork and other ways to improve care. It set up a fund to pay for preventive care, to test new kinds of pricing reform, such as auctions and bidding, and experiment with new forms of community care. By contrast, there has been little innovation in these sorts of areas in either the private or public sectors in South Africa.
In SA, the NHI debate in public has until recently focused almost exclusively on finance issues. The recently published White Paper on NHI is still dominated by the financing issues but begins to acknowledges the need to reform delivery. In the public sector, weak systems of leadership and clinical governance are noted, and quality problems in the areas of staff attitudes, waiting times, cleanliness, drug stock-outs, infection control, and safety and security of staff and patients. The lack of a coherent unified health information management system, and increased patient loads compromise the quality of care. It is noted that the public’s discontent with the quality of services has escalated medico-legal claims in both the public and private sectors. Job design, performance management systems, remuneration policies, employment relationships, inhospitable physical work environment, shortages of equipment and other tools of trade, workplace culture and human resource practices, facility workforce planning and career-paths are all major issues. In response to these many issues, certification of providers to quality standards is frequently mentioned, and re-engineering of primary care (e.g. the so-called Ideal Clinic) is promoted as the basis for better delivery, but relatively few details are offered.
We should learn from Obamacare – by addressing integration of care, emphasising quality, and encouraging a range of innovations, with relevant measurable outcomes. Ideas for how this may be achieved will be covered in a future blog post.
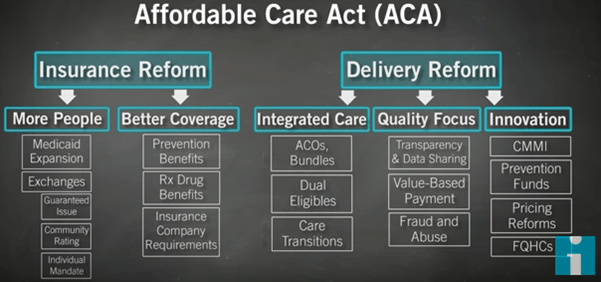
Figure 1. ACA and AHCA: Don Berwick Breaks It Down. https://www.youtube.com/watch?v=KoTOzNRw8bg – accessed July 8, 2017
Get an email whenever we publish a new thought piece
The ICHOM 2023 Conference took place in Barcelona this year and was the largest gathering on Value-Based Health Care (VBHC) worldwide. Attended by leading industry experts representing countries from all
2.5 min read

By Insight. "When we die, our bodies become the grass, and the antelope eat the grass. And so we are all connected in the great Circle of Life." – Mufasa
8 min read

Meet our experts
Author

More Insights
Focused Thought Pieces