Considerations on the new COVID variant.
18 January 2021
5.8 min read
By Craig Getz and Gareth Kantor
South Africa is experiencing a second wave of the COVID-19 pandemic. In the last ten days, over 140,000 new cases and more than 4,000 COVID-19 related deaths have been reported. The second wave is believed to be driven by the so-called South African variant of SARS-CoV-2 (501.V2).
Concerns have been raised that the new variant spreads more rapidly and results in higher levels of morbidity and mortality including amongst the young who have been relatively insulated from severe disease. There are also questions as to whether vaccines, which have been shown to be effective in preventing COVID-19, will be as effective against this variant.
These uncertainties are having significant ramifications. Several countries have closed their borders to South Africa. Domestically, the anxiety around COVID-19 has risen. We urgently need to deepen our understanding of the new variant. This will enable a reduction in alarmist messaging and mediate between the conflicting expert opinions which dominate our public discourse.
Inferences on the impact of the new variant are available through the study of medical schemes data. This data is available in real-time and provides a reliable record of newly diagnosed infections, hospital admissions and deaths. This data can be used to determine whether the arrival of the new variant has coincided with an increase in case fatality rates. The results presented herein are derived from a sample of medical schemes for which Insight is monitoring the pandemic.
Case fatality rates refer to the proportion of confirmed cases which result in death. Case fatality rates use positive PCR tests as the basis for confirmed cases. This differs from infection fatality rates. Infection fatality rates refer to the proportion of total infections which result in death.
Case fatality rates are considered as the total number of persons infected is not known with any level of precision. This is because persons with no or mild symptoms are unlikely to be tested. Case fatality rates may be affected by the availability of tests, testing protocols and the propensity of the population to undergo testing. As such, case fatality rates may be influenced by matters other than the inherent characteristics of the virus.
The KwaZulu Natal Research Innovation and Sequencing Platform (KRISP) has suggested that the new variant has become dominant since November 2020 ¹. We can make inferences about the impact of the new variant by contrasting the experience before and after November 2020.
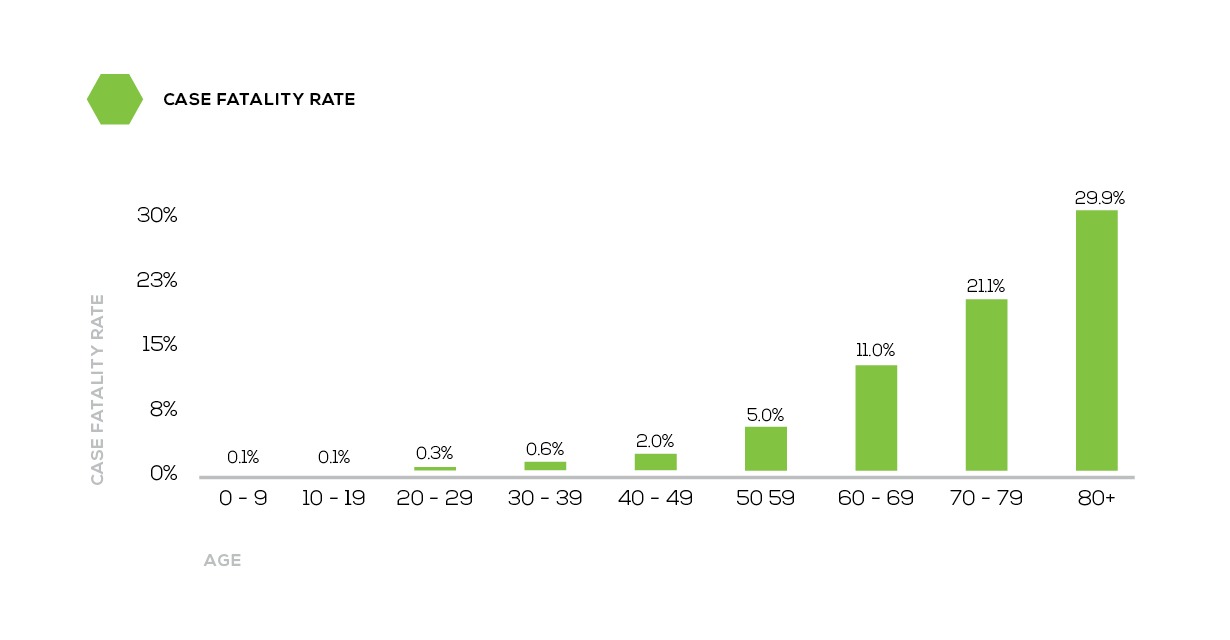
Case fatality rates can change in response to variations in the profile of the population infected. For example, Covid-19 is fatal far more often in the elderly. Over age 80 the case fatality rate is almost 30%, under age 40 it is 0.6% or less. This is a 50-fold difference. All things equal, if more elderly persons are infected, case fatality rates will rise.
Figure 1:
Case fatality rates by age
Age is not the only factor which impacts on case fatality rates. Our data has confirmed that male gender and various comorbidities (including but not limited to diabetes, hypertension and HIV) are significant drivers of morbidity and mortality. These factors are accounted and adjusted for when tracking trends using actuarial risk adjustment techniques.
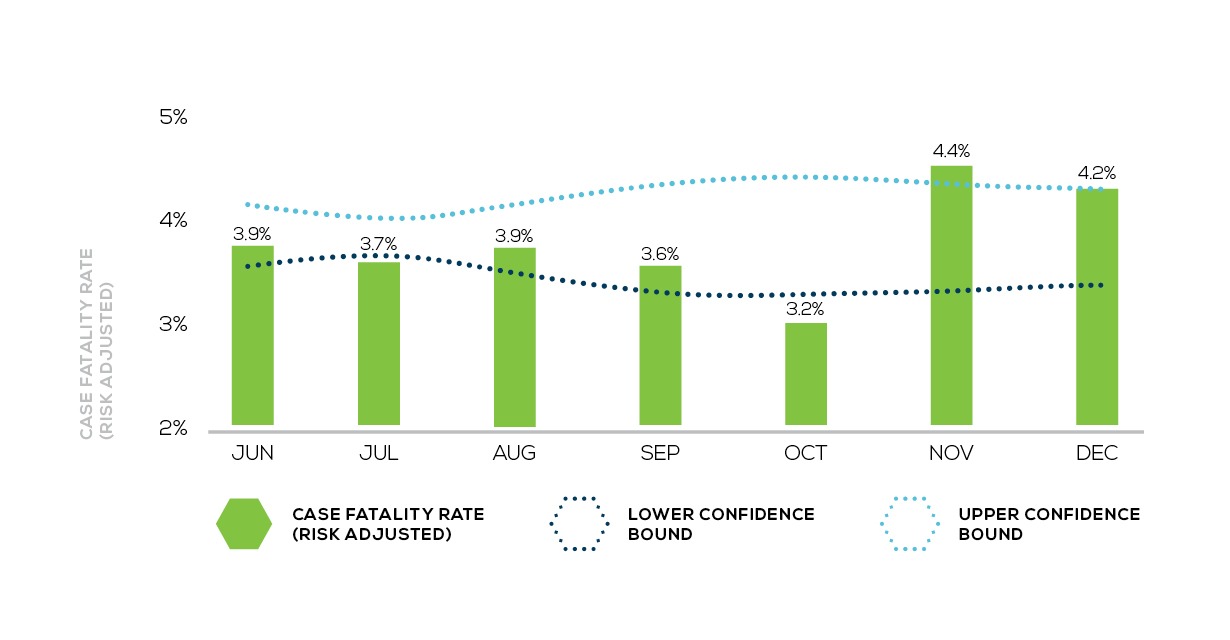
Prior to November, the risk adjusted case fatality rate ranged from 3.2% to 3.9%. (Experience before June is not shown due to insufficient data volumes). Since November, the case fatality rate has increased to 4.4% in November and 4.2% in December. This is outside the 95% confidence interval which suggests that the increase is statistically significant rather than a function of expected, random month-to-month variability.
Figure 2:
Trends in case fatality rates²
 Whilst the increase in the case fatality rate is of concern, one cannot conclude that the increase is the result of the new variant, alone or in part. It may be the result of changes in other factors such as increased pressure on hospital capacity or strained testing capacity which results in less severely ill patients going undiagnosed.
Whilst the increase in the case fatality rate is of concern, one cannot conclude that the increase is the result of the new variant, alone or in part. It may be the result of changes in other factors such as increased pressure on hospital capacity or strained testing capacity which results in less severely ill patients going undiagnosed.
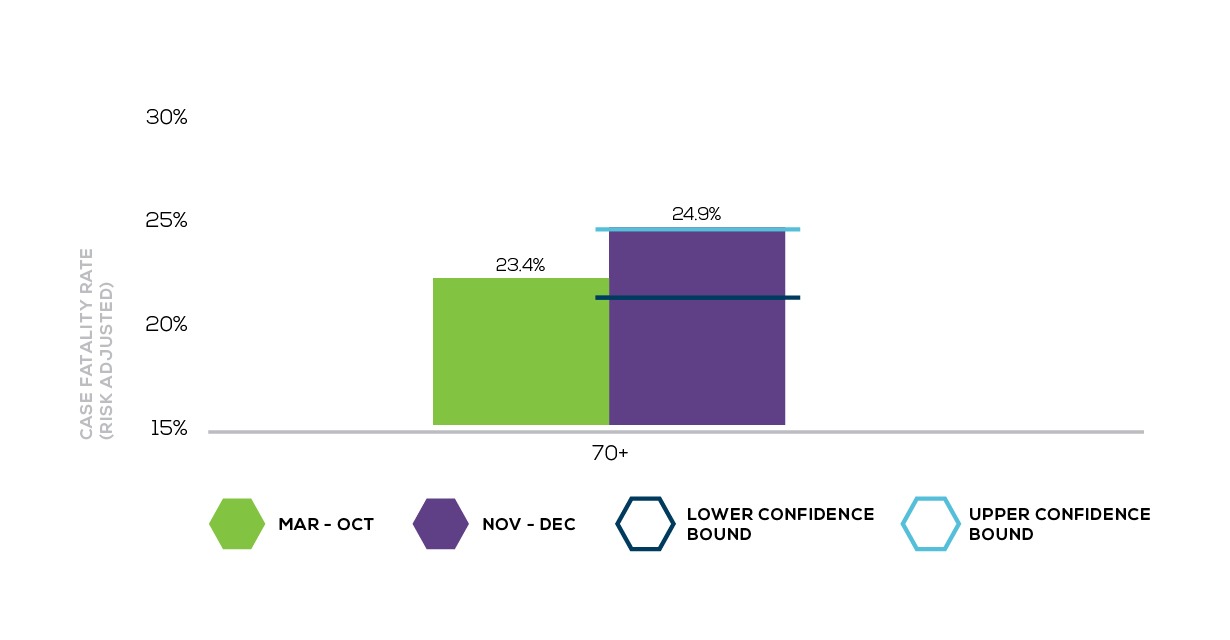
Higher risk-adjusted case fatality rates are evident across age bands. These increases are not, however, statistically significant (except in the age band 50 – 59). This does not support the contention that the new variant is causing significantly more severe disease in younger individuals.
Figure 3:
Trends in case fatality rates by age (age 0 to 49)
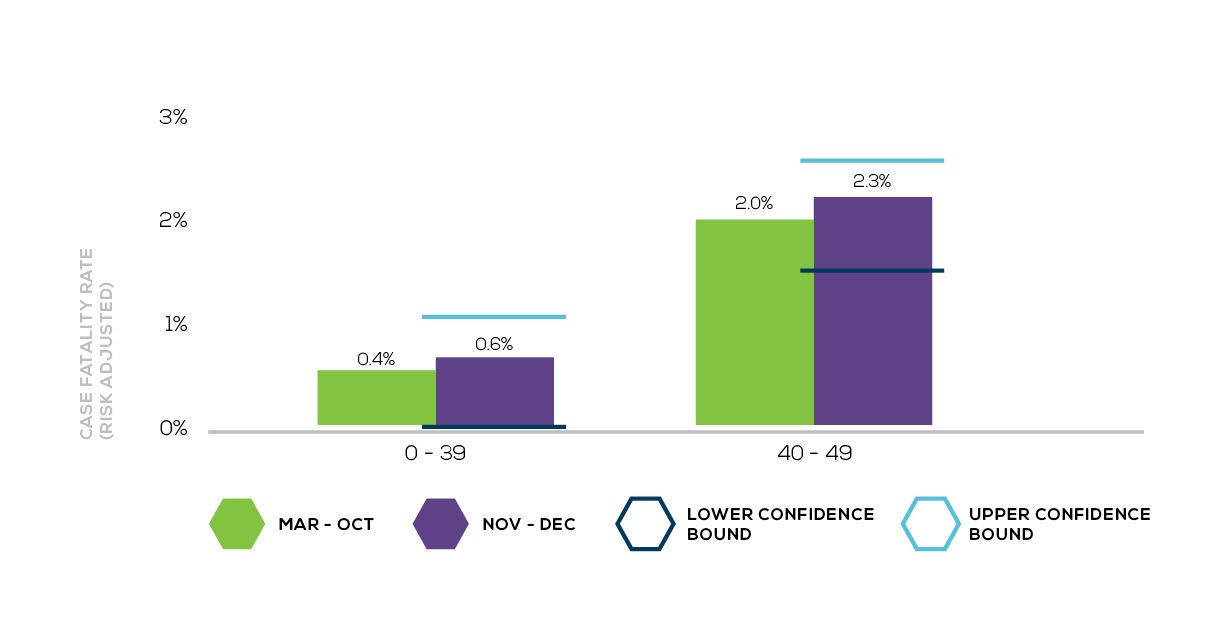
Figure 4:
Trends in case fatality rates by age (age 50 to 69)
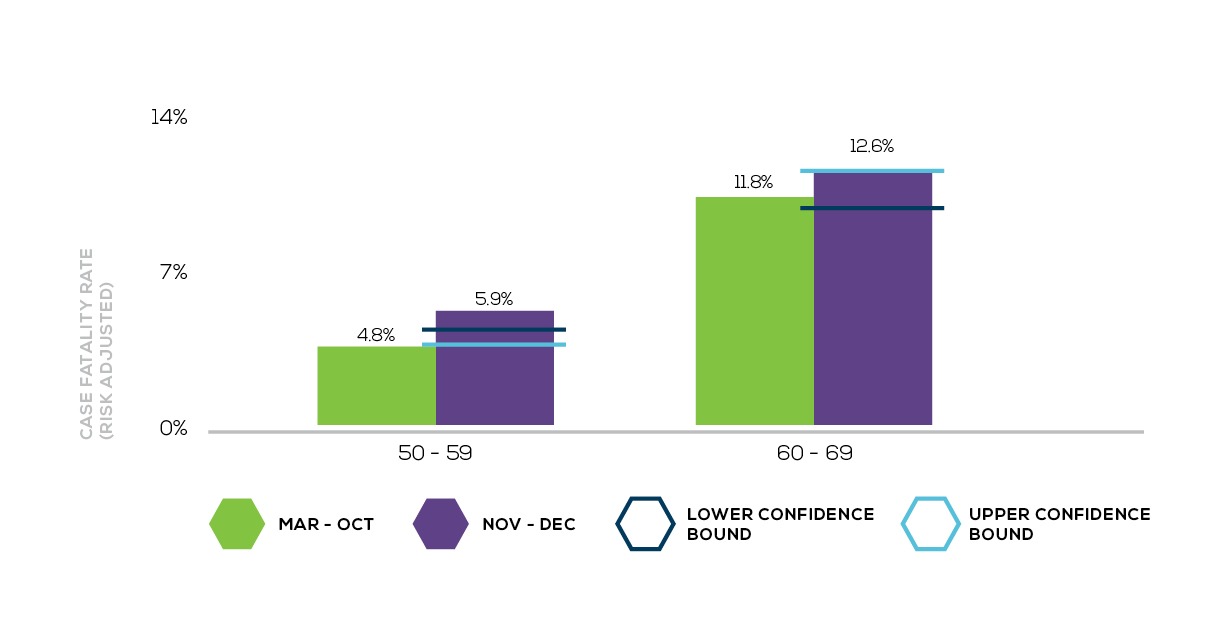
Figure 5:
Case fatality rate (over age 70)
 The COVID-19 pandemic has taught us not to draw conclusions prematurely. It is too early to say exactly what impact the new variant is having on morbidity and mortality. Whilst the early signs are worrisome, results are not conclusive. Case fatality rates may be distorted by testing capacity and other such extenuating factors. The early signs highlight the importance and the urgent need for further investigations, using high quality clinical and system level data so that definitive conclusions can be made.
The COVID-19 pandemic has taught us not to draw conclusions prematurely. It is too early to say exactly what impact the new variant is having on morbidity and mortality. Whilst the early signs are worrisome, results are not conclusive. Case fatality rates may be distorted by testing capacity and other such extenuating factors. The early signs highlight the importance and the urgent need for further investigations, using high quality clinical and system level data so that definitive conclusions can be made.
¹ https://www.nicd.ac.za/new-variant-of-sars-cov-2-frequently-asked-questions/
² The lower bound of the confidence interval had been breached in previous months (particularly in October). It is postulated that this was the result of improved treatment protocols.
Get an email whenever we publish a new thought piece
The ICHOM 2023 Conference took place in Barcelona this year and was the largest gathering on Value-Based Health Care (VBHC) worldwide. Attended by leading industry experts representing countries from all
2.5 min read

By Insight. "When we die, our bodies become the grass, and the antelope eat the grass. And so we are all connected in the great Circle of Life." – Mufasa
8 min read

Meet our experts
Author

More Insights
Focused Thought Pieces