It’s Complicated
19 April 2016
11.6 min read
The first round of public hearings held by the Health Market Inquiry during February and March of this year have, at the same time, been both fascinating and frustrating to watch.
I certainly don’t envy the panel members. There is an enormous amount of information to process. This includes thousands of pages of written submissions, presentations and transcripts. It is the task of the inquiry to process all of this information, distil it down to the facts and then make recommendations. This is by no means an easy task: not all of the information provided by stakeholders is relevant to the terms of reference of the inquiry and will need to be filtered out.
A wide range of diagnoses of the problems ailing the healthcare industry have been put forward. These diagnoses were strongly influenced by the points of view of the stakeholders making presentations, and there is an unmistakeable emotional undertone. The level of animosity between different stakeholders is conspicuous.
What I found frustrating was the general quality of the information presented. Some rather weighty accusations were made based on little more than anecdotal evidence, selectively chosen to make a particular point. We shouldn’t lose sight of the experience of the patients, who are the most important stakeholders of all. The natural way for such individuals to share their experiences is by telling their stories. Unfortunately, the submissions of several other organisational stakeholders also relied on unsubstantiated narratives rather than hard data. This is no way to establish the truth and develop a solution, particularly when dealing with something as vital as healthcare. To quote W. Edwards Deming: “In God we trust, all others bring data”.
The healthcare system is an interplay of competing forces that seek to have their interests presented. These interests are not only economic in nature. Patients want quality care and to be treated with compassion. They want to be able to conveniently access the provider of their choice. Medical scheme members want their medical schemes to pay their claims. At the same time, they want to pay low contributions. Healthcare providers would like to have their expertise recognized and object to having medical schemes prescribe how they should treat patients by means of managed care, protocols and formularies. They want to be compensated fairly for their services, in a timely manner. Medical schemes are desperately trying to balance the books without passing on ever-higher contribution increases, a seemingly unattainable goal. Regulators are trying to achieve a number of different objectives such as enforcing regulations, protecting patients, ensuring the sustainability of the industry and expanding equitable access to healthcare.
Most stakeholders, in making their diagnoses and proposing remedies, also did not consider the realities faced by other stakeholders or anticipated how they may react. “This party does a thing that we don’t like and we propose this measure that will prevent them from doing that.” Unfortunately, the nature of the healthcare system means that such a simplistic problem solving approach is not going to serve us well.
We naturally think that, if we change system X and start following process Y then the result will predictably be Z. This is not how the world, and healthcare in particular, works. Why not? Most people would concede that there is no other system that is more complex or less predictable than healthcare.
“Complexity” was a recurring theme of the hearings and this word was used hundreds of times. What is the reason for this? After all, to paraphrase a question asked by the chairperson of the inquiry panel: what is so complex or complicated about a person getting sick and accessing the treatment they need?
This is certainly not a new question. A simple internet search produced a number of articles considering the nature, causes and implications of complexity in healthcare.
Before continuing we need to establish what we mean when we say “complex”. This article (2) points out that the definition of the word is often ambiguous, subjective and dependent on the context where it is used. The authors choose to define complexity in terms of how interrelated the components of the system are, with interrelatedness meaning how much system components influence each other. A complex system is therefore one with a large number of components that are highly interrelated.
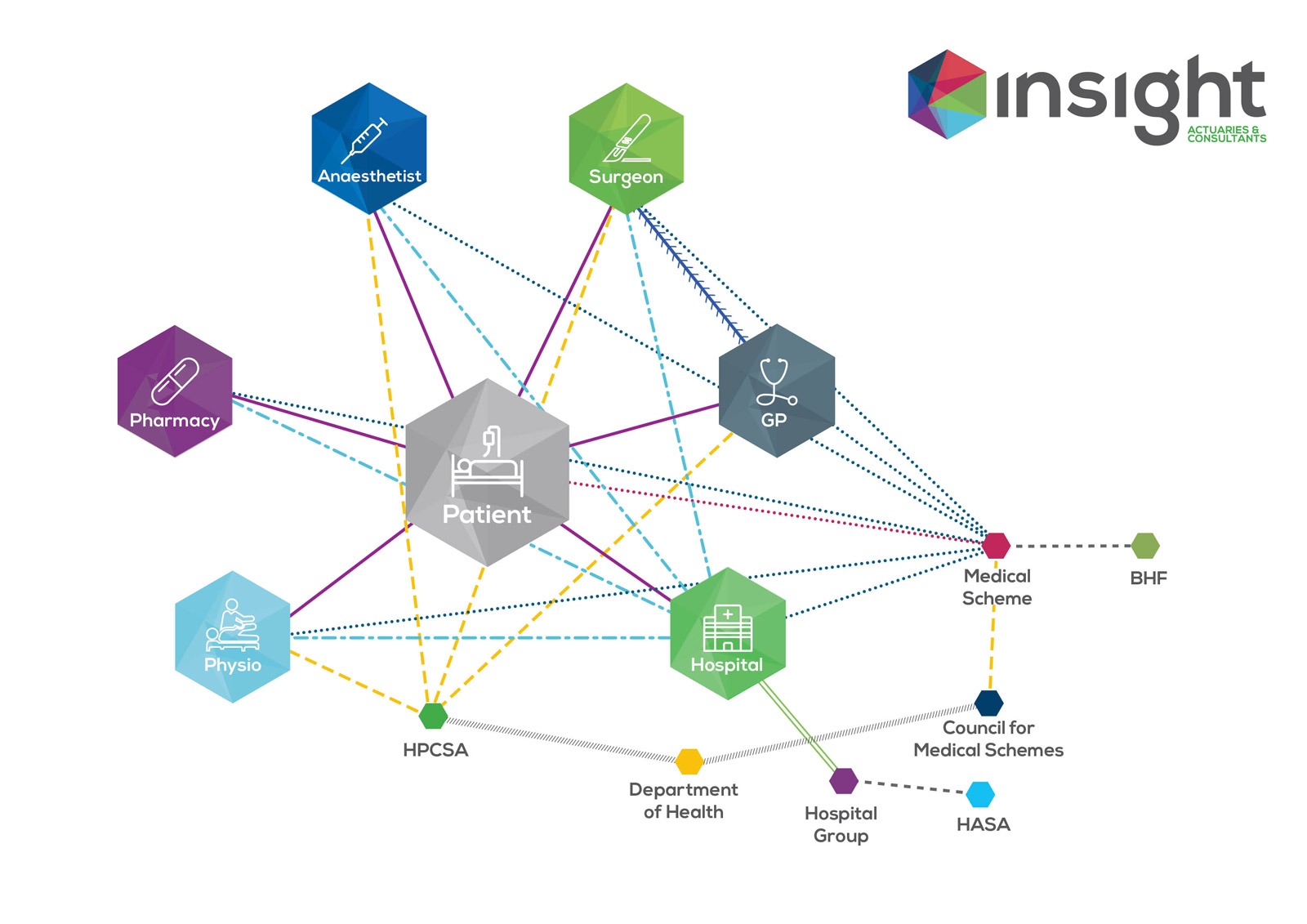
This definition certainly applies to the South African private healthcare system. Consider a patient admitted for a simple procedure. This patient interacts with the hospital, nurses, the surgeon and an anaesthetist. In addition, the patient may have interacted with a GP that referred them to the surgeon in the first place, a radiologist and/or pathologist to confirm a diagnosis, a physiotherapist to aid recovery after the procedure, the pharmacy that dispensed the necessary medication and potentially many more healthcare providers. Each of these providers compete with other providers. If the patient belongs to a medical scheme, then the patient and each service provider interacts with a medical scheme (or the scheme’s administrator or managed care organisation) in order to get their claims paid. Each provider belongs to a representative body and is regulated in some way. The regulatory bodies may be answerable to higher authorities. They all interact with each other in complicated ways.
For example, if the medical scheme does not pay the claims resulting from the example above, in full, there will be a reaction. The patient may consider changing to a different option or to another medical scheme. They may lay a complaint against the medical scheme with the Council for Medical Schemes. They will share their unhappiness with other people, influencing opinion and decision making. A provider, tired of having to manage bad debts, may decide to demand that patients pay them directly, leaving the patient responsible for recovering the amount from the medical scheme. In response the medical scheme may revise its rules or change its benefits, setting off another round of action and reaction.
If we try to visualize all of this, we need to draw a complex diagram with a lot of circles representing the role-players and many lines connecting them to represent the interactions. More essentially these are not simple one-way interactions. Scale the diagram up from a single patient to the entire healthcare system and the resulting diagram becomes appallingly complex.
A consequence of this is that we cannot always predict what the ultimate impact of an intervention in the system will be with a high degree of certainty. This doesn’t mean that it isn’t possible to understand the system or plan for the future. You can even plan decades ahead, but if you think you will only have to do it once you are mistaken. Useful analysis of the system is still possible so long as we simplify our description of the system by ignoring weak interrelations but taking all the meaningful ones into account. Our problem is that many voices seem to be happily ignoring these interrelations altogether.
Joe Flowers (3) provides a very good explanation of the unpredictability arising from this complexity. He lists the following consequences of seeing healthcare as a complex system:
You get what you pay for. If we incentivise stakeholders based on specific desirable outcomes, then we will get more of those outcomes. However, this is not an independent linear relationship. Outcomes that have nothing to do with those that we are trying to influence will be affected. Also, priorities change and resources are reallocated in response to changing incentives.
The Law of Unintended Consequences reigns supreme. To the closest approximation, the most significant consequences of any given intervention will be the unintended ones. For example, co-payments that are intended to discourage unnecessary utilisation of healthcare will also discourage necessary healthcare.
Controlling specific cost and utilization becomes a game of Whack-A-Mole. For example, if we strictly control behaviour in a certain setting then treatment may be shifted to another setting in order to escape these controls.
Systemic decisions reflect the needs and desires of the individual decision-makers, not the system as a whole or even sectors within the system. These needs and desires will be strongly influenced by incentives. As a result, we shouldn’t expect anyone to automatically” do the right thing, particularly when the system incentivises them to act differently.
The consequence of all these interrelations is that many of the properties of the system can be described as “emergent”. Wikipedia defines emergence as a process whereby larger entities, patterns, and regularities arise through interactions among smaller or simpler entities that themselves do not exhibit such properties. A famous example of emergence is Langton’s Ant, which shows how a very simple set of rules can result in complex behaviour. The most important implication of Langton’s Ant is that, even though it is based on very simple rules, you cannot easily predict how the system will evolve. The easiest way to see how the process will evolve is to allow it to run and see what happens.
Private healthcare in South Africa can be described as a complex adaptive system which displays a specific type of emergence: self-organising behaviour. The system looks the way it does because it organised itself in response to various interventions (or the lack of intervention) in a context defined by regulation, economic and other constraints, the need to survive and the desire to thrive. The architects of the system could not have anticipated that their decisions would have this specific outcome.
This phenomenon or emergence and unpredictability has important implications for any efforts to reform private healthcare in South Africa, whether it is intended to fix the private healthcare system or to bring about universal healthcare. Firstly, there really are no simple solutions. Secondly, any approach to “design” a blueprint of an ideal healthcare system in the same way as a Boeing 787 or a factory production line and then implementing it is unlikely to result in the planned outcomes.
Rather than trying to solve all of our healthcare problems in a single stroke based on some grand plan we need to consider all of the complexity, design and implement incremental reforms, monitor the outcomes and then adapt. Continuously.
References
- Health Market Inquiry (http://www.compcom.co.za/healthcare-inquiry/)
- Thomas G. Kannampallil, Guido F. Schauer, Trevor Cohen, Vimla L. Patel (2014). Considering complexity in healthcare systems.
- Flower J (2009). Health Care as a Complex Adaptive System. http://www.imaginewhatif.com/health-care-as-a-complex-adaptive-system/
- Google search “why is healthcare so complex?”
Get an email whenever we publish a new thought piece
The ICHOM 2023 Conference took place in Barcelona this year and was the largest gathering on Value-Based Health Care (VBHC) worldwide. Attended by leading industry experts representing countries from all
2.5 min read

By Insight. "When we die, our bodies become the grass, and the antelope eat the grass. And so we are all connected in the great Circle of Life." – Mufasa
8 min read

Meet our experts
Author

More Insights
Focused Thought Pieces