Application of the Insight Diagnosis Related Grouper (Part 2)
A Diagnosis Related Grouper (DRG) is a tool which to categorise hospital admissions into statistically homogenous and clinically intuitive categories.
10 August 2023
6.8 min read
Photo by Markus Winkler | Unsplashed
A Diagnosis Related Grouper (DRG) is a tool which to categorise hospital admissions into statistically homogenous and clinically intuitive categories. Statistical homogeneity refers to the extent to which the admissions within each DRG are associated with similar costs per admissions and similar levels of resource utilisation. Statistical homogeneity implies that DRGs can explain variations in costs per admissions and resource utilisation per admission.
The ability to establish statistically homogenous groupings and to explain variations in costs per admission and resource utilisation per admission is central to several fundamental DRG applications. This includes the facilitation of provider benchmarking and the underpinning of alternative reimbursement models. This begs the question as to the degree to which the classifications produced by the Insight DRG are statistically homogeneous. Simply put, how good is the Insight DRG?
There are various ways to objectively assess the degree to which DRGs are statistically homogenous. The R-squared measure (R2) is the most considered. The R-squared measure indicates the proportion of variance in a dependent variable which can be explained by an independent variable. In the context of hospitalisations, it refers to the extent to which variations in costs per admission and resource utilisation per admission can be explained by DRGs.
The R-squared measure ranges between 0% and 100%. A higher R-squared is indicative of a greater ability to explain variation. For example, an R-squared of 50% would indicate that DRGs explain half of all the variability in hospital costs per admission whilst an R-squared of 100% would indicate that DRGs explain all the variability in hospital costs per admission. To achieve an R-squared of 100%, every admission within a DRG would have to have precisely the same hospital costs.
Asking what is the minimum R-squared which indicates that a DRG is sufficiently good at explaining variations in hospital costs per admission can be likened to the cliché of asking how long is a piece of string. The answer is that it depends. It depends on a multitude of factors. This includes what alternatives are available for classifying hospital admissions, what types of hospital admissions are being classified and what purpose the DRG is being applied for.
Additionally, a low R-squared is not always indicative of an inability to robustly categorise hospital admissions. Cost variations and low R-squared values could be a function of extraneous factors. This includes differences in the tariff rates billed by different hospitals for the same services and differences in the clinical treatment pathways followed by different healthcare practitioners.
The Rand Corporation (a renowned American research institute) has studied the explanatory power for various DRGs in the United States in the context of Medicare hospital costs per admission. Rand observed adjusted R-squared values of up to 44% depending on which grouper was used[1]. This provides something of a benchmark whilst noting that there may be many reasons why Medicare hospital costs per admission may be either more or less variable than their South African equivalents.
Based on 2022 hospital admissions across the Insight data universe, the Insight DRG achieves an adjusted R-squared of 45% with respect to hospital costs per admission prior to trimming. The R-squared ranged between 44% and 48% depending on the funder considered. In this way, the Insight DRG performs similarly when compared with its American equivalents per the Rand study. The limitations of such comparisons must, however, be stressed.
Every DRG can be assigned to a Major Diagnosis Category (MDC). An MDC is a classification which reflects the bodily system to which an admission pertains. Adjusted R-squared values are calculated for each MDC. Similarities between the Insight DRG and its American equivalents are again evident. Most notably, the Insight DRG is associated with a significantly higher R-squared in the context of pregnancy, childbirth and the puerperium and diseases and disorders of the eye but a lower R-squared in the context of diseases and disorders of the circulatory system.
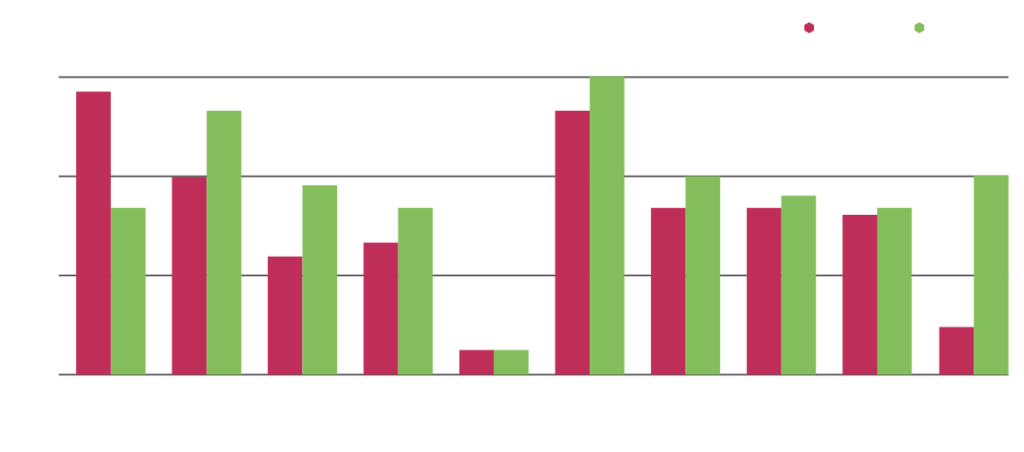
Figure 1: R-squared by MDC (top 10 by volume)
The statistical homogeneity of DRGs is lessened by outliers. Outliers refer to admissions with either exceptionally high or low costs per admission, given the DRG to which they are assigned. Outliers are typically the results of either incomplete or incorrect clinical coding (which results in inaccurate DRGs classifications) or less commonly exceptional complications or comorbidities.
Outliers have the potential to distort key DRG applications such as provider benchmarking exercises and alternative reimbursement models and should be removed accordingly. Outliers are typically removed via a statistical process known as trimming. Insight employs the interquartile approach trimming such that approximately 5.0% of admissions are deemed to be outliers and removed from. After trimming, the adjusted R-squared increases to 68% across the Insight data universe.
Statistical homogeneity can be increased further by recognising that some DRGs are poorly suited to benchmarking and alternative reimbursement models based on hospital costs per admission but well suited to benchmarking and alternative reimbursement models based on hospital costs per day[2]. DRGs with coefficients of variance above 0.85 and standard deviations above R65,000 (prior to trimming) with reference to the cost per admission are deemed to fit this criterion.
After this amendment, the adjusted R-squared increases to 88% across the Insight data universe.
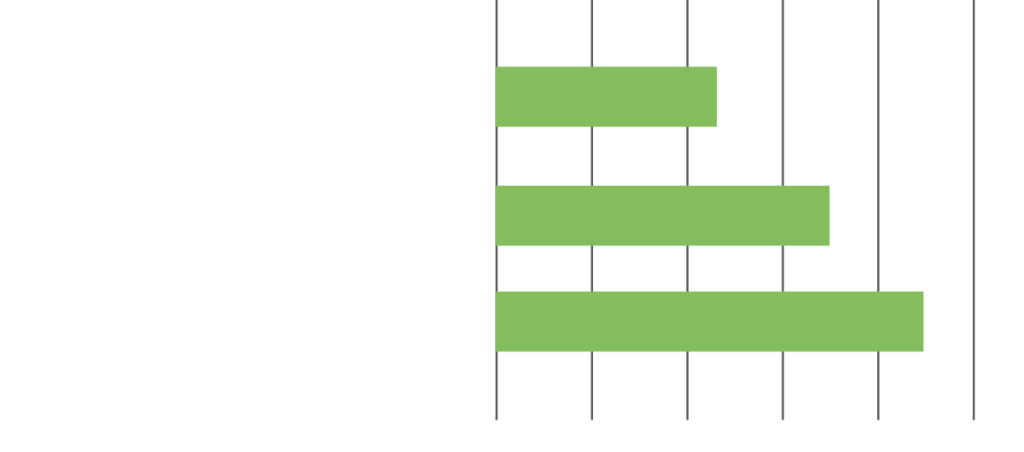
Figure 2: R-squared with and without trimming
The Insight DRG compares well with international norms and achieves an exemplary R-squared, particularly when it is judiciously applied. This suggests that the Insight DRG is more than sufficient to facilitate robust provider benchmarking and to underpin alternative reimbursement models.
Nonetheless, the DRG remains subject to ongoing improvement and development. We welcome feedback from all stakeholders, be it hospital groups, healthcare professionals, healthcare funders and their managed care organisations, on how to further enhance the Insight DRG.
[1] https://www.rand.org/content/dam/rand/pubs/working_papers/2008/RAND_WR606.pdf
[2] When Insight considers the costs per day, day one is upweighted in view of the fact that the first day of a hospital admission is typically associated with disproportionately high costs. For surgical admissions, the first day is weighted at four and half days. For non-surgical admissions the first day is weighted at two and half days.
Get an email whenever we publish a new thought piece
The Insight DRG was introduced in 2013 and quickly went on to be the most widely used DRG in the South African market. A key part of ensuring the DRG
3 min read

A Diagnosis Related Group (DRG) is a tool with which to classify hospital admissions into clinically intuitive and statistically homogenous categories. Clinical intuitiveness means that categorisations can be easily understood
6.7 min read

Meet our experts
Author
More Insights
Focused Thought Pieces