If You Want to Understand Prostate Cancer Treatment Outcomes, Ask Patients!
Prostate cancer gets much less public attention than breast cancer, but in the US, 1 in 8 men will develop this disease in their lifetime, and two to three of them will die from it.
11 October 2022
5 min read
According to the Council for Medical Schemes, the corresponding lifetime prevalence in South Africa is lower – 1 in 19. Still, prostate cancer is the leading cause of cancer death among men in sub-Saharan Africa. Movember Day (1 November) helped raise public awareness of prostate cancer but, sadly, is no longer commemorated in SA.
The most common risk factor for prostate cancer is increasing age. Genes play a role, too; the risk of getting and/or dying from prostate cancer increases with a family history of prostate cancer. African ancestry approximately doubles the risk, which ought to make prevention and treatment a national priority.
Early detection should help. The PSA (Prostate-Specific Antigen) test was introduced decades ago, but mass PSA screening led to overdiagnosis, overtreatment and recommendations against routine testing of all healthy men. PSA testing may best be focused on a narrower age range (55-69 years) and patients with additional risk factors.
Fortunately, treatment advances, including better chemotherapy drugs and robotic surgery, have improved outcomes. Ultrasound and MRI are imaging methods that now provide important information for prognosis and treatment.
For men who get prostate cancer, survival matters, obviously, but the loss of sexual, bowel and urinary function are potential treatment side-effects that can occur along with cure and extension of life. These issues can be hard to discuss but are very important to men and their partners. Urine and blood flow are measurable, but patients need to report their symptoms, level of function, and preferences, for use in decision-making.
Shared decision-making is particularly important in prostate cancer because of multiple treatment options, including
- surgery, either ‘open’ abdominal or perineal operations or robotic prostatectomy;
- radiation; and
- medication (androgen deprivation and chemotherapy).
Treatments may have trade-offs (side effects versus survival) that patients (and their doctors) need to consider. Watchful waiting (‘active surveillance’) is an option because some prostate cancers grow very slowly; many older men die with the disease, not of the disease.
Patient-reported outcomes (PROs) are validated measurement tools that can help answer at least three important questions:
- “How am I compared with before treatment?” The patient’s PRO results are compared with the pre-treatment state to assess the effects of treatment.
- “How am I compared with patients like me?” The patient’s PRO results are compared with similar patients, which can help with treatment choice.
- “What can I expect in the future?” PRO trends provide information about prognosis.
The UK (National Prostate Cancer Audit (NPCA)) and Australasian (Prostate Cancer Outcomes Registry of Australia and New Zealand (PCOR-ANZ) prostate cancer registries use PROs, such as EPIC-26, to track treatment experience and to examine outcome variation across different treatment centres and between different treatment types.
EPIC-26 is a PRO tool with 26 questions specific to prostate cancer treatment. Each response is given a score, and then specific groups of scores are aggregated into separate domains to produce summary scores for urinary incontinence, urinary irritation/obstruction, and bowel and sexual function. A score of 100 represents the best possible function. One or two-point differences are usually not significant, but minimum clinically important differences that patients are likely to notice have been defined for sexual function (10-12 points), urinary incontinence (6-9 points), urinary irritation (5-7 points), and bowel function (4-6 points).
Separately, patients are asked, “how big a problem has your [sexual function/urinary function/bowel habits] been over the last four weeks?” This reflects how ‘bothered’ they are with their function. The most recent (2021) Australian PCOR-ANZ report was based on nearly 21,000 responses 12 months after treatment or diagnosis. Sexual function was the domain where most men reported the most bother, particularly after surgery (45%). Major bowel bother was least reported, more commonly for radiation and systemic therapy than for surgery. Urinary incontinence was more common for patients in the surgical category than the other two forms of treatment. See Figures 1 and 2 below.
As we begin offering PROs and PROMs (patient-reported outcome measures) to more medical schemes and other clients in South Africa, we will encourage clinicians to use PROs to facilitate better clinical decision-making that hopefully will lead to treatment results reflecting what matters most to patients and families.
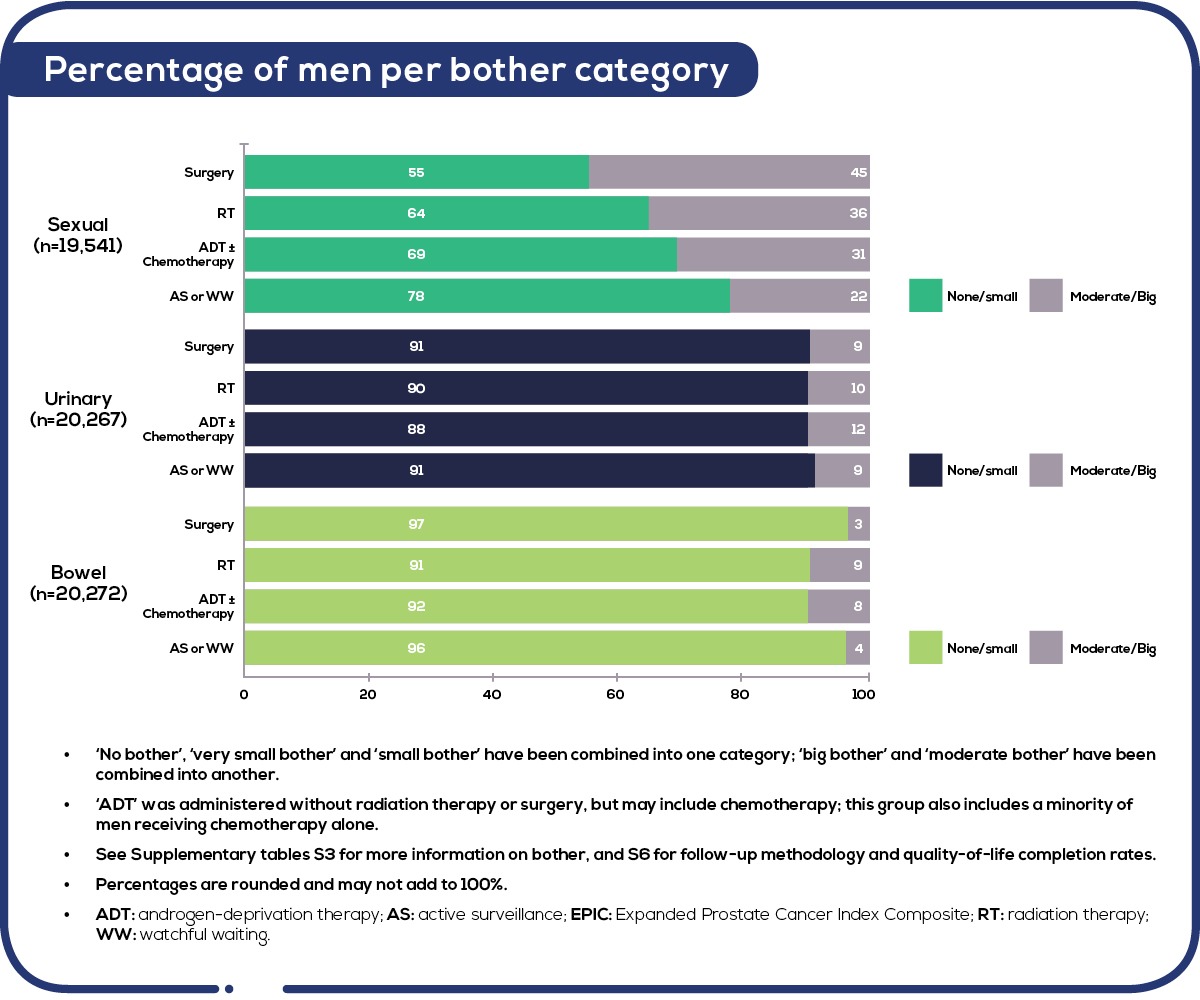
Figure 1: Patient-reported bother, 12 months after treatment, by EPIC-26 domain and treatment type (2015-18). Source: PCOR-ANZ prostate cancer registry, annual report, 2020, page 26 – report
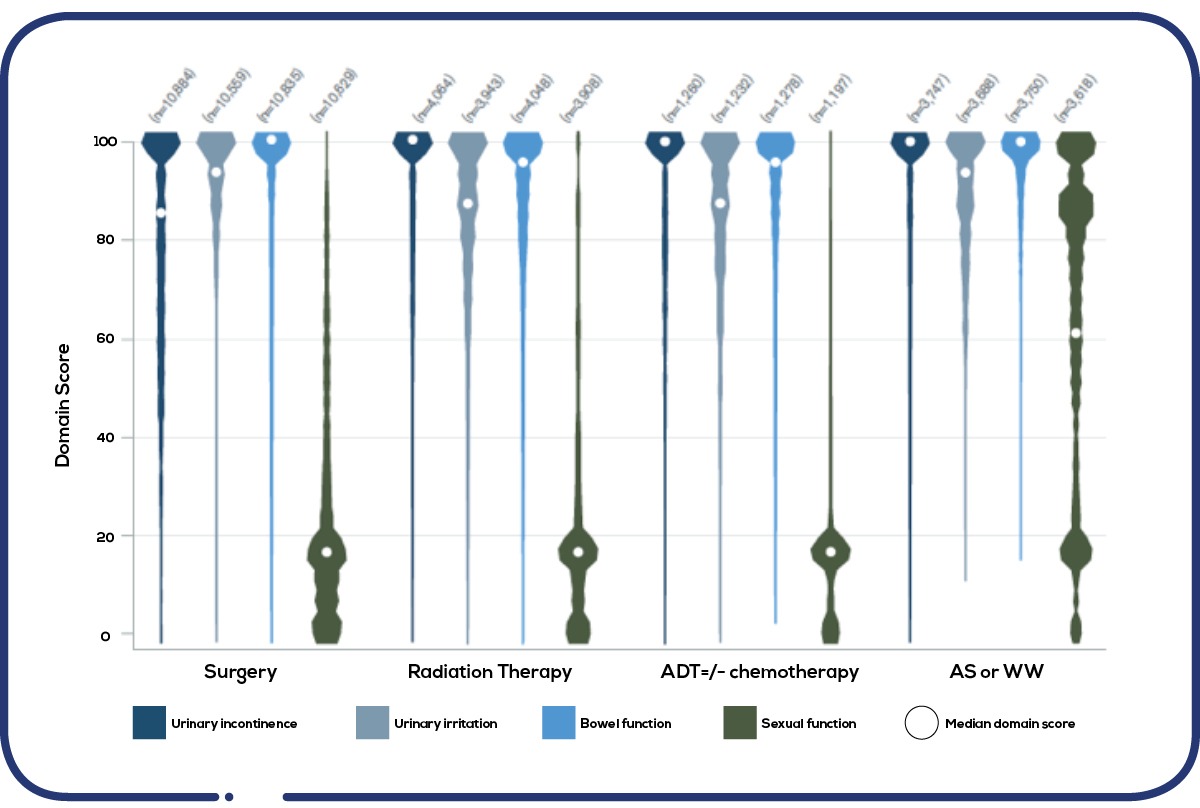
Figure 2: Distribution of responses to the function domains of the EPIC-26 PROMS questionnaire. Source: PCOR-ANZ, annual report, 2020, page 27 – report
Get an email whenever we publish a new thought piece
Hypertension care is often a series of disconnected events. Blood pressure is measured, advice is given, a prescription is written, and follow-up is advised. The patient disappears back into everyday
8.2 min read

If hypertension is common, measurable and treatable, why do so many patients still have uncontrolled blood pressure? Drug shortages, diagnostic challenges or a lack of treatment guidelines are not the
10.6 min read
Meet our experts
Author

More Insights
Focused Thought Pieces